ARCHIVED
![]() To Contents
To Previous Page To Next Page
To Publications Page To
Home Page
To Contents
To Previous Page To Next Page
To Publications Page To
Home Page

|
National Drug Intelligence Center National Drug Threat Assessment 2003 January 2003 Cocaine and CrackCocaine is a principal drug threat to the United States. Both powder cocaine and crack are prevalent throughout the country, and overall availability is stable at high levels. All Drug Enforcement Administration (DEA) Field Divisions, High Intensity Drug Trafficking Areas (HIDTAs), as well as most Pulse Check sources, report that powder cocaine and crack are readily or widely available, and most describe cocaine as the greatest drug threat to their areas.1 National Drug Threat Survey (NDTS) data show that 33.1 percent of state and local law enforcement agencies nationwide identify cocaine--both powder and crack--as their greatest drug threat. Statistical reporting regarding cocaine-related federal investigations, arrests, and seizures did not change appreciably from 2000 to 2001. The demand for powder cocaine and crack is relatively stable at high levels and possibly rising slightly among adults. Estimated cocaine production increased in 2001; however, estimates suggest that only about 28 percent of the export-quality cocaine prepared for shipment to world markets was smuggled into the United States, primarily through the Mexico-Central America corridor. Cocaine is transported via commercial and private vehicles, rail traffic, buses, pedestrians, as well as commercial and private aircraft. The distribution of powder cocaine and crack is pervasive throughout the country, and the market for both forms of the drug appears to be stable overall. All DEA Field Divisions and HIDTAs report that powder cocaine is widely distributed in their areas, and most report that crack cocaine also is widely distributed in inner cities, particularly in lower income areas. Primary market areas for cocaine include Atlanta, Chicago, Houston, Los Angeles, Miami, and New York. NDTS data indicate that 8.2 percent of state and local law enforcement agencies nationwide identify powder cocaine as their greatest drug threat.2 Regionally, more state and local law enforcement agencies in New England (15.5%), the Florida/Caribbean (12.9%), and the Great Lakes (11.1%) identify powder cocaine as the greatest threat than do those in the Mid-Atlantic (8.9%), New York/New Jersey (8.9%), Southwest (7.9%), and Southeast regions (6.4%). Powder cocaine was identified as the greatest threat by only 3.5 and 0.7 percent of agencies in the West Central and Pacific regions.3 NDTS data further reveal that 24.9 percent of state and local law enforcement agencies nationwide identify crack cocaine as their greatest drug threat. Regionally, more state and local law enforcement agencies in the Southeast (55.3%) and Florida/Caribbean (47.8%) identify crack cocaine as the greatest threat than do those in the Mid-Atlantic (27.0%), Great Lakes (25.9%), New York/New Jersey (20.6%), and Southwest regions (14.7%). Crack cocaine was identified as the greatest threat by 10.9, 8.5, and 2.7 percent of agencies in the New England, West Central, and Pacific regions, respectively. Contributing to the threat posed by cocaine, users of the drug experience many short- and long-term physical effects. Short-term effects include increased heart rate, blood pressure, and body temperature as well as tremors, vertigo, muscle twitches, and paranoia. Other consequences of cocaine use include chaotic heart rhythms, seizures, and strokes. Long-term use, especially via intranasal administration, may lead to loss of sense of smell, nosebleeds, throat irritation, and deterioration of the nasal septum, while prolonged use via ingestion can cause bowel gangrene resulting from decreased blood flow. The American Heart Association reports that long-term use also can cause aortic dissection (a tearing in the lining of, or rupturing of, the aorta), a condition that may result in death. Violence and collateral criminal activity often are associated with the distribution and use of cocaine, crack cocaine in particular. Law enforcement reports that rivalries between distribution groups, especially gangs, account for most cocaine-related violence, much of which involves increases in homicides, armed robberies, and assaults when distributors of crack cocaine move into new market areas.4
AvailabilityPowder cocaine is readily available throughout the country, and availability appears to be stable overall--rising slightly in some areas and declining slightly in others. All DEA Field Divisions and HIDTAs, as well as most Pulse Check sources, report that powder cocaine is readily or widely available in their areas. According to NDTS data, 76.2 percent of state and local law enforcement agencies nationwide report that the availability of powder cocaine is high or medium, while 21.6 percent describe it as low.5 Agencies in the Mid-Atlantic (89.6%) and New England regions (85.9%) account for the greatest proportions reporting high or medium availability, while those in the West Central (68.9%) and Pacific regions (56.8%) account for the smallest. The availability of crack cocaine appears to be stable overall. Reporting from DEA Field Divisions and HIDTAs suggests that crack is readily available in major cities--although not at the high levels of the early 1990s--and is available to a lesser extent in many smaller cities and towns.
NDTS data show that 67.1 percent of state and local law enforcement agencies nationwide describe the availability of crack cocaine as high or medium, while 27.2 percent describe it as low. Agencies in the Southeast (92.7%) and Florida/Caribbean regions (87.1%) account for the greatest proportions reporting high or medium availability. Agencies in the West Central (44.7%) and Pacific regions (40.4%) again account for the smallest proportions. The percentages of OCDETF investigations and indictments for powder cocaine and crack were higher than for any other drug. Of 1,334 OCDETF investigations initiated in fiscal year (FY) 2001, 65.1 percent involved powder cocaine and 25.3 percent involved crack cocaine. Also, of 3,787 OCDETF drug indictments obtained in FY2001, 33.6 percent referenced powder cocaine as the primary drug and 29.8 percent referenced crack. The number of DEA arrests involving cocaine dropped from 15,767 in 2000 to 12,847 in 2001, accounting for approximately 40 and 34 percent, respectively, of all DEA arrests in those years. Data from the U.S. Sentencing Commission (USSC) show the percentages of federal drug sentences involving powder and crack cocaine were nearly unchanged from FY2000 to FY2001. During that period, federal drug sentences involving powder cocaine declined only slightly from 23 to 22 percent, while those involving crack held steady at 21 percent. Cocaine seizures between 2000 and 2001 were relatively stable as well. Data from the Federal-wide Drug Seizure System (FDSS) indicate that the amount of cocaine seized declined from 106,621 kilograms in 2000 to 105,864 kilograms in 2001.6 DEA reports that cocaine prices throughout the country were low and stable in 2001. Nationally, the wholesale price for a kilogram of powder cocaine ranged from $10,000 to $36,000, while price ranges for ounce and gram quantities ranged from $400 to $1,800 and from $20 to $200, respectively. In 2001 the average nationwide purity of powder cocaine was 69 percent for kilogram quantities and 56 percent for gram quantities. Prices for crack cocaine ranged nationally from $3 to $50 per rock (1/10 g to 1/2 g), with prices generally ranging from $10 to $20.
DemandThe demand for powder and crack cocaine is relatively stable at high levels and possibly rising slightly among adults. National Household Survey on Drug Abuse (NHSDA) data show that among all users (12 and older) the rate of past year use (use at least once in the preceding 365 days) increased significantly for powder cocaine from 1.5 percent in 2000 to 1.9 percent in 2001.7 Past year use of crack cocaine also increased from 0.3 to 0.5 percent during the same period. National-level prevalence studies indicate rising cocaine use among adults. NHSDA data show that the rate of past year cocaine use among young adults aged 18-25 increased significantly between 2000 and 2001 from 4.4 to 5.7 percent for powder cocaine and from 0.7 to 0.9 percent for crack. For adults aged 26-34 past year use was relatively stable but rose slightly for both powder cocaine (2.1% to 2.7%) and crack (0.4% to 0.6%). Past year use rates also rose slightly for adults aged 35 and older between 2000 and 2001 from 0.7 to 0.9 percent for powder cocaine and 0.2 to 0.3 percent for crack cocaine. Data from the Monitoring the Future (MTF) survey show that cocaine use among adults was statistically unchanged between 2000 and 2001.8 For MTF respondents aged 19-28 past year use of powder cocaine rose from 4.8 percent in 2000 to 5.3 percent in 2001, while past year crack use rose slightly from 1.2 to 1.3 percent; however, neither change is statistically significant. Among college students aged 19-22, MTF data show that past year use of powder cocaine held at 4.1 percent in both 2000 and 2001 and that past year use of crack cocaine in 2001 was at 0.9 percent for the third consecutive year. National-level prevalence studies indicate that adolescent cocaine use appears to be stable to declining overall. According to NHSDA data, 1.5 percent of those aged 12-17 reported past year cocaine use in 2001 compared with 1.7 percent in 2000. In 2001 past year use of crack was reported at 0.4 percent for the third consecutive year. MTF data show relative stability in past year use of cocaine among students. In 2001 and 2002 past year use rates for powder cocaine were 1.9 and 1.8 percent, respectively, for eighth graders and 3.0 and 3.4 percent for tenth graders; rates for twelfth graders were 4.4 percent in both years. In those years rates of past year use for crack cocaine were mostly stable for eighth (1.7% and 1.6%) and twelfth graders (2.1% to 2.3%) but increased significantly for tenth graders (1.8% to 2.3%). Data from the Parents' Resource Institute for Drug Education (PRIDE) show stability in cocaine use for younger students and sharp declines among older students.9 Between the 2000-2001 and 2001-2002 school years, past year cocaine use held steady for junior high students at 2.1 percent. Past year use decreased significantly, however, for both senior high students (5.5% to 5.1%) and twelfth graders (7.9% to 7.1%). National studies that track the attitudes of adolescents toward drug use show little change between 2000 and 2001 regarding cocaine. According to the Partnership Attitude Tracking Study (PATS), the percentage of seventh through twelfth graders who agreed there was great risk in using powder cocaine or crack regularly held steady between 2000 and 2001 at 82 percent.10 The percentage who saw great risk in trying powder cocaine or crack once or twice increased--but just slightly--from 47 percent in 2000 to 48 percent in 2001. MTF data indicate that students' perceptions of powder and crack cocaine use were statistically unchanged from 2001 to 2002. In 2002 the proportions of students perceiving great risk in trying powder cocaine once or twice were 43.2, 51.3, and 49.5 percent for eighth, tenth, and twelfth graders, respectively. The proportions of students perceiving great risk in trying crack cocaine once or twice were 47.4, 57.4, and 50.8 percent for eighth, tenth, and twelfth graders. The most recent data available regarding the consequences of cocaine use reveal rising emergency department (ED) mentions and declining treatment admissions. Data from the Drug Abuse Warning Network (DAWN) show that the estimated number of cocaine-related ED mentions increased significantly from 174,881 in 2000 to 193,034 in 2001.11 Data from the Treatment Episode Data Set (TEDS) show that the number of admissions to publicly funded treatment facilities for cocaine use (smoked and nonsmoked) declined from 244,051 in 1998 to 228,206 in 1999, the latest year for which such data are available.12 The proportion of admissions for which cocaine was the primary substance of abuse declined as well from 15.1 percent in 1998 to 14.4 percent in 1999. Almost three-quarters (73%) of all cocaine-related admissions in 1999 were attributed to crack, or smoked, cocaine. TEDS data also reveal the use of cocaine in combination with other illegal drugs. Marijuana, methamphetamine, and heroin were the secondary drugs of abuse most often mentioned in 1999 TEDS admissions for which cocaine was identified as the primary substance of abuse. One common trend reported in both DAWN ED and TEDS data is the rising average age of cocaine users. DAWN ED data show significant increases between 2000 and 2001 in ED cocaine mentions for patients aged 35 and older (+14.4%) and for patients aged 55 and older (+19.7%). TEDS data further indicate that in 1999 most cocaine-related treatment admissions were in the 35-39 age category, when in 1998 most cocaine-related treatment admissions were in the 30-34 age category. The typical admission to publicly funded treatment facilities in 1999 for nonsmoked cocaine use was male (66%), Caucasian (49%), and between 35 and 39 years old (22%); the typical admission for smoked cocaine use was male (58%), African American (58%), and between 35 and 39 years old (26%). Data from the Arrestee Drug Abuse Monitoring (ADAM) program show that past year use of powder cocaine was reported by 12.5 percent of adult male arrestees in 2001, down from 13.4 percent in 2000.13 Past year use of crack cocaine was reported by 18.9 percent of adult male arrestees in 2001, up from 17.5 percent in 2000. In 2001 the median percentage of males testing positive for cocaine (both powder and crack) was 29.1 percent; only marijuana was detected more often (42.7%).
ProductionCocaine production increased sharply between 2000 and 2001. Interagency estimates indicate that potential cocaine production--occurring primarily in Colombia, Peru, and Bolivia--increased from 805 metric tons (100% pure) in 2000 to 930 metric tons (100% pure) in 2001. Intensified eradication programs have contributed to declines in net coca cultivation since 1995 in Peru (-71%) and Bolivia (-59%) but have failed to offset increases in Colombia, where net coca cultivation has increased 234 percent. At least three-quarters of the coca cultivated for processing into cocaine is grown in Colombia, and Colombian drug trafficking organizations control most cocaine production. According to the Interagency Assessment of Cocaine Movement (IACM), in 2001 an estimated 823 metric tons of export-quality cocaine (average 78% pure) were potentially available to depart South America for worldwide markets. The purity of export-quality cocaine is derived from DEA laboratory analysis of wholesale-level cocaine seized in the United States.
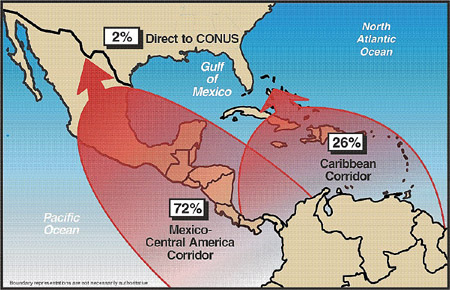
TransportationCocaine is transported to the United States via the Mexico-Central America corridor, via the Caribbean corridor, and directly from South America. The IACM reports that 521 metric tons of cocaine were detected departing South America moving toward the United States in 2001. An estimated 191 metric tons were seized or consumed en route, leaving an estimated 330 metric tons of cocaine available to U.S. markets in that year. Of that amount, most (72%) transited the Mexico-Central America corridor, 26 percent transited the Caribbean corridor, and 2 percent was transported directly to the United States (see Figure 5). These percentages vary somewhat from transport activity in 2000, when approximately 66 percent of the cocaine transited the Mexico-Central America corridor, 31 percent transited the Caribbean corridor, and 3 percent was transported directly to the United States.
Mexico-Central America CorridorCocaine is transported through the Mexico-Central America corridor primarily via the eastern Pacific and western Caribbean maritime routes. Colombian drug trafficking organizations used the eastern Pacific route heavily in 2001: according to the IACM, more than half (52%) of all cocaine detected en route to the United States in that year transited the eastern Pacific. Traffickers using this route transport cocaine primarily by fishing vessels and go-fast boats from the west coast of Colombia to rendezvous points off the coast of Mexico. The cocaine is then moved ashore, usually in Mexico, on vessels controlled by Mexican drug trafficking organizations. The western Caribbean route accounted for approximately 19 percent of all cocaine detected en route to the United States in 2001. When using this route Colombian traffickers transport cocaine primarily by go-fast boats from the north coast of Colombia through the western Caribbean to Central America or Mexico. Once the cocaine is in Mexico, it is supplied to Mexican traffickers who use overland vehicles and small aircraft to transport the drug to the U.S. border. Cocaine is smuggled across the border via commercial and private vehicles, rail traffic, buses, pedestrians, and private aircraft. Nearly 80 percent of the cocaine seized at ports of entry (POEs) along the U.S.-Mexico border in 2001 was seized at the Calexico (2,346 kg) and San Ysidro (990 kg) POEs in California; the Nogales (1,399 kg) POE in Arizona; and the Laredo (1,032 kg), Hidalgo (597 kg), and El Paso (587 kg) POEs in Texas. Seizure data from the El Paso Intelligence Center (EPIC) show that Calexico, San Ysidro, and Nogales also ranked among the top Southwest Border POEs in amounts of cocaine seized in 2000. California led the Southwest Border states in cocaine seized at POEs in 2000 (3,388 kg) and 2001 (3,530 kg); however, cocaine seizures at Texas POEs increased significantly from 1,628 kg in 2000 to 3,362 kg in 2001. Texas led in cocaine seized between POEs with 255 and 516 kilograms seized, respectively, in those years. Texas also accounted for the vast majority of the cocaine seized at checkpoints and through traffic stops in 2000 (7,366 kg) and 2001 (5,991 kg). Cocaine smuggled into the United States through the California POEs of Calexico and San Ysidro most often is transported to Los Angeles for local consumption and for further transport to cocaine markets throughout the United States. Cocaine smuggled through the Nogales POE usually is destined for Central Arizona (Phoenix and Tucson), the primary market areas of Chicago and Los Angeles, and smaller markets throughout the Pacific, Southwest, and West Central regions. Cocaine smuggled into the United States through the Texas POEs of El Paso, Hidalgo, and Laredo typically is destined for Chicago, Dallas, Houston, and New York.
Caribbean CorridorColombian drug trafficking organizations and Bahamian, Dominican, Haitian, Jamaican, and Puerto Rican criminal groups transport cocaine to the United States through the Caribbean corridor often transiting Jamaica, Haiti, the Dominican Republic, and the Lesser Antilles in the eastern Caribbean. According to the IACM, criminal groups increased their use of Jamaica and Haiti as transshipment points for cocaine en route to U.S. and other world markets in 2001. Colombian transporters use commercial and noncommercial sea and air transportation--often in combination--to transport cocaine to the United States through the Caribbean. Cocaine is transported primarily by maritime conveyances such as go-fast boats, containerized cargo, and coastal freighters and by couriers on commercial flights. Dominican, Haitian, Jamaican, and other criminal groups often are employed to complete the final transportation phase, smuggling the cocaine into the United States through a number of POEs in the eastern United States. The primary POEs for cocaine smuggled into the eastern United States by commercial maritime and air transportation are in Florida, New York, and Puerto Rico. EPIC seizure data for 2001 show commercial maritime cocaine seizures of 2,579 kilograms in Miami, 895 kilograms in Ft. Lauderdale, 336 kilograms in San Juan, and 314 kilograms on Staten Island. The POEs at Miami and Ft. Lauderdale also led commercial maritime seizures in 2000 with 3,992 and 1,260 kilograms of cocaine seized, respectively, in that year. According to HIDTA reporting, cocaine is transported to these POEs primarily via containerized cargo, although shipments frequently are transported via coastal freighters to Miami and by fishing vessels to Puerto Rico. Cocaine also is transported via go-fast boats to Puerto Rico and other islands. POEs in Miami, New York, and Puerto Rico also report frequent seizures of cocaine from couriers on commercial flights, often traveling from South America but also from other countries. According to EPIC, commercial air cocaine seizures in 2000 and 2001 were highest in Miami (2,115 kg and 1,527 kg) and New York (571 kg and 814 kg). Seizures at POEs in Puerto Rico followed: the Aguadilla POE accounted for 456 kilograms of cocaine seized in 2000 and the San Juan POE for 264 kilograms in 2001. Cocaine smuggled through these POEs generally is destined for markets in the eastern half of the United States. Cocaine is transported from Miami to Atlanta, New York, and Philadelphia; from New York to Atlanta, Chicago, Detroit, Philadelphia, and Washington, D.C.; and from Puerto Rico to New York and Philadelphia.
Direct to the Continental United StatesAccording to the International Narcotics Control Strategy Report (INCSR), Colombian traffickers smuggle cocaine from Colombia directly into major Atlantic and Gulf Coast POEs, primarily on commercial vessels or commercial flights. But as mentioned previously, this direct route accounted for only 2 percent of all cocaine transported to the United States in 2001. The INCSR further reports that the U.S.-sponsored Port Security Program appears to have significantly reduced not only commercial but also noncommercial maritime transportation of cocaine directly to the United States.
DistributionThe distribution of powder cocaine and crack occurs throughout the country, and the market for the drug appears to be stable overall. All DEA Field Divisions and HIDTAs report that powder cocaine is widely distributed in their areas, and most report that crack cocaine also is widely distributed in inner cities, particularly in lower income areas. Mexican criminal groups control most wholesale cocaine distribution in the western United States, and their influence in eastern markets--traditionally controlled by Colombian and Dominican criminal groups--appears to be growing. Every DEA Field Division in the Pacific, Southwest, and West Central regions reports that Mexican wholesale and midlevel distributors are predominant. Mexican distributors also control most wholesale cocaine distribution in Chicago and New Orleans and have become much more prominent in New York, often working directly with Colombian and Dominican groups in these cities. Colombian and Dominican criminal groups control wholesale cocaine distribution in the Florida/Caribbean, Southeast, Mid-Atlantic, New York/New Jersey, and New England regions. In the western United States only the DEA Houston and Los Angeles Field Divisions report a significant presence of Colombian wholesale distributors. A wide range of criminal groups and independent dealers distribute cocaine at the retail level. African American and Hispanic gangs control most retail distribution of powder cocaine throughout the country. Mexican criminal groups are prominent retail distributors of powder cocaine in the Pacific, West Central, Southwest, and Great Lakes regions, while retail distributors of Colombian, Dominican, and Puerto Rican origin are prominent in many eastern states. DEA and HIDTA reporting indicates that Hispanic independent retail distributors, who often receive supplies of powder cocaine from several different sources, are common in western states, particularly in the Pacific region. Caucasian independent distributors are pervasive in all regions and often are responsible for much of the midlevel and retail distribution of powder cocaine in suburban and rural areas. African American and Hispanic gangs control most retail distribution of crack cocaine in every region of the country. Retail crack distribution typically occurs in inner-city, lower income housing units and sometimes at open-air drug markets, where it frequently is sold along with powder cocaine or other drugs such as heroin and, to a much lesser extent, MDMA. Wholesale amounts of powder cocaine generally are distributed in 1-kilogram bricks sealed in plastic or cellophane. Retail amounts (1/8 g to 1 g) typically are packaged in small plastic bags, cellophane, glassine, or paper. Powder cocaine typically is converted to crack cocaine at or near distribution sites and is distributed in rocks (1/10 g to 1/2 g); retail packaging for crack is the same as for powder cocaine.
Primary Market AreasCocaine is distributed and used in every region of the country. Reporting from law enforcement and public health agencies indicates, however, that Atlanta, Chicago, Houston, Los Angeles, Miami, and New York are the primary market areas because of high levels of use and because they serve as centers for the national-level distribution of wholesale quantities of cocaine to other markets. Baltimore, Boston, Central Arizona (Phoenix and Tucson), Detroit, Newark, and Philadelphia are significant cocaine markets, but the levels of use within and distribution from these areas are not as great as in the primary market areas.
Atlanta. Atlanta is a primary market area for cocaine. Law enforcement reporting indicates a growing population of illicit drug users in the Atlanta area, most of whom use powder cocaine and crack. Moreover, the consequences of cocaine use are high or increasing. The Community Epidemiology Work Group (CEWG) reports that 70.3 percent of treatment admissions in Atlanta in 2000 involved powder cocaine (22.5%) or crack (47.8%).14 DAWN data show that the estimated number of cocaine-related ED mentions increased significantly (+42.7%) from 6,229 mentions in 2000 to 8,891 mentions in 2001. Atlanta had the third highest rate of ED mentions among DAWN cities, behind Chicago and Philadelphia, at 244 per 100,000 population. DAWN mortality data for Atlanta show that cocaine was mentioned in 173 of 259 deaths involving drug abuse in 1999 and in 151 of 233 deaths in 2000.15 It was listed as the primary drug of abuse in 65 of 82 single-drug deaths in 2000. According to 2000 ADAM data, nearly half (49%) of adult male arrestees in Atlanta tested positive for cocaine, the most for any ADAM site in 2000. DEA and HIDTA reports indicate that Mexican and, to a lesser extent, Colombian and Dominican distributors control wholesale distribution of cocaine in Atlanta. Cocaine is transported to Atlanta primarily from the U.S.-Mexico border (often via Houston) and Florida. Mexican criminal groups are the primary distributors of powder cocaine at the wholesale level in the Atlanta area, directly supplying African American and Hispanic gangs who control retail crack distribution. Law enforcement reporting and seizure data indicate that Atlanta-based wholesale and midlevel distributors supply cocaine to drug markets in the Mid-Atlantic and Southeast regions as well as in Texas. Chicago. The Chicago HIDTA reports that several tons of cocaine are transported to Chicago annually both for local consumption and for further distribution to other markets throughout the Midwest. Consequent to that local consumption, the estimated number of ED cocaine mentions in Chicago rose from 14,879 in 2000 to 16,202 in 2001. DAWN data also show an increase between 2000 and 2001 in the rate of ED mentions for cocaine from 246 to 277 per 100,000--the most for any DAWN reporting city. DAWN mortality data for Chicago show that cocaine was mentioned in 456 of 878 deaths involving drug abuse in 1999 and in 499 of 869 deaths in 2000. It was the drug of abuse in 120 of 268 single-drug deaths in 2000, the most for any drug in Chicago. According to 2001 ADAM data, 40.6 percent of adult male arrestees in Chicago tested positive for cocaine, second only to New York in that year. DEA and HIDTA reports indicate that Mexican wholesale cocaine distributors are predominant in Chicago, although Colombian wholesale distributors are active as well. Most cocaine is transported to Chicago via tractor-trailers and private vehicles from Southwest Border POEs. Chicago-based street gangs such as Gangster Disciples, Latin Kings, and Vice Lords control most retail distribution of powder cocaine and crack in the city. These gangs sell powder cocaine and crack in open-air markets, public housing projects, private residences, and gang-controlled communities. Law enforcement reporting and seizure data from EPIC indicate that Chicago-based wholesale distributors supply powder cocaine and crack to markets throughout the Great Lakes region and, occasionally, to some areas of the Mid-Atlantic, Southeast, and West Central regions. Houston. Consequences likely occasioned by high levels of cocaine use (especially crack), and the distribution of multiple-ton quantities of cocaine to other U.S. drug markets, render Houston a primary market area. National-level drug data sources such as DAWN, CEWG, and Pulse Check do not report on Houston; however, the Texas Commission on Alcohol and Drug Abuse (TCADA) closely tracks statistics associated with the consequences of cocaine use in the state. According to TCADA, cocaine is the most abused drug in the Houston area. Crack cocaine was the primary drug of abuse mentioned in 1,628 of 5,508 adult admissions to TCADA-funded treatment programs in Harris County (Houston area) in 2001, the most for any drug. Powder cocaine was the primary drug of abuse mentioned in 305 admissions. According to ADAM data, 31.5 percent of males arrested in Houston in 2000 tested positive for cocaine. According to DEA and HIDTA reporting, cocaine is transported to Houston in multikilogram and ton quantities for local and national distribution. Mexican wholesale distributors transport the drug primarily overland via the U.S.-Mexico border, while Colombian wholesalers typically use couriers on commercial flights and commercial vessels arriving at ports in or near Houston to transport cocaine. Mexican, Colombian, Jamaican, and Dominican criminal groups, as well as local gangs, distribute cocaine at the retail level. DEA reports indicate that wholesale quantities of powder cocaine are distributed from Houston to regional markets, such as Dallas-Ft. Worth, and to other primary market areas, such as Atlanta, Chicago, and New York. In addition, EPIC seizure data show Houston as the origin of cocaine shipments to the Great Lakes and Southeast regions, to Miami, and to cities in Missouri, Pennsylvania, and Rhode Island. Crack cocaine is distributed from Houston to regional markets in Texas, Louisiana, and Mississippi. Los Angeles. Information from DEA, HIDTA, and Pulse Check reporting indicates that the cocaine market in Los Angeles is large and stable. In addition, multiple tons of cocaine are distributed from the city to markets throughout the country. DAWN data show a rise in the estimated number of ED mentions for cocaine in Los Angeles from 9,094 in 2000 to 9,999 in 2001. The rate of ED mentions for cocaine also rose from 105 to 117 per 100,000 population between 2000 and 2001. DAWN mortality data for Los Angeles show that cocaine was mentioned in 544 of 1,887 deaths involving drug abuse in 1999 and in 471 of 1,192 deaths in 2000. Mortality data further note that cocaine was listed as the drug of abuse in 136 of 295 single-drug deaths in 2000. Mexican wholesale distributors control most cocaine distribution in Los Angeles, although Colombian wholesale distributors are present as well. DEA and HIDTA reporting indicates that Mexican and Colombian wholesale and midlevel distributors supply cocaine to local Hispanic gangs (such as Mexican Mafia and 18th Street) and African American gangs (such as Bloods and Crips), who dominate street-level distribution of both powder cocaine and crack. Independent dealers distribute cocaine at the retail level as well. Gangs and independent dealers often sell powder cocaine, typically in multigram and ounce quantities, on street corners and in hotel rooms in urban and suburban neighborhoods. Mexican and Colombian criminal groups distribute multiple tons of cocaine from Los Angeles to every region of the country including to other primary market areas such as Atlanta, Chicago, and New York. Miami. Miami is among the largest cocaine markets in the country. HIDTA reporting indicates that cocaine is the greatest drug threat to the Miami area and that use of both powder cocaine and crack continues to rise. DAWN data indicate that the estimated number of ED mentions for cocaine rose from 4,383 in 2000 to 4,641 in 2001. DAWN data also show that from 2000 to 2001 the rate of ED cocaine mentions held steady at 225 per 100,000. DAWN mortality data indicate that cocaine was mentioned in 130 of 167 deaths involving drug abuse in Miami in 1999 and in 151 of 216 deaths in 2000. It also was listed as the drug of abuse in 25 of 27 single-drug deaths in 2000. According to 2000 ADAM data, 43.5 percent of adult male arrestees in Miami tested positive for cocaine. Colombian wholesale distributors control most cocaine distribution in Miami, although Haitian wholesale distributors are prominent as well. Colombian and Haitian midlevel distributors supply powder cocaine to local retail distributors, primarily Haitian, Jamaican, and Mexican criminal groups and African American and Hispanic gangs. Haitian and Jamaican criminal groups and African American and Hispanic gangs control retail distribution of crack cocaine in Miami. Caucasian independent dealers also distribute crack but to a lesser extent. Multiple tons of powder cocaine are distributed from Miami to markets in the Great Lakes, Mid-Atlantic, New England, New York/New Jersey, and Southeast regions including to the primary market areas of Atlanta, Chicago, and New York. New York. New York remains a primary market area for cocaine, despite some indications that the consequences of cocaine use are declining. The estimated number of DAWN ED mentions for cocaine, both powder and crack, decreased from 14,250 in 2000 to 13,898 in 2001; the rate of ED mentions per 100,000 population was 166 in both years. According to DAWN mortality data, cocaine was mentioned in 394 of 729 deaths involving drug abuse in New York in 1999 and in 492 of 924 deaths in 2000, when it was listed as the drug of abuse in 196 of 284 single-drug deaths. ADAM reports that 44.6 percent of adult male arrestees in New York tested positive for cocaine in 2001, still the highest percentage for any ADAM site in that year, despite decreasing from 46.0 percent in 2000. Colombian and Dominican wholesalers control most cocaine distribution in New York, although Mexican wholesale distributors are becoming more prominent. Colombian, Dominican, Mexican, and Puerto Rican criminals are the principal midlevel cocaine distributors, and they supply retail distributors who typically are African American and Hispanic gangs. African American, Jamaican, and Puerto Rican criminals control most retail distribution of crack cocaine in the city. New York-based wholesale and midlevel cocaine distributors supply powder cocaine to markets throughout the Great Lakes, Mid-Atlantic, New England, New York/New Jersey, and Southeast regions including to the primary market areas of Atlanta and Chicago.
Key DevelopmentsAccording to DEA's Cocaine Signature Program, the average purity of wholesale cocaine departing South America for the United States declined from 86 percent in 1998 to 78 percent in 2001. Several factors can influence wholesale purity. The Attorney General's Cocaine Availability Working Group reports, however, that the most plausible are a shortage of the chemical solvents and oxidizers used to refine cocaine (such as potassium permanganate) and efforts to stretch cocaine supplies to meet growing demand in markets in Central and South America and Europe. The decline in overall wholesale cocaine purity may be affecting the purity of retail cocaine. DEA reports that retail purity levels also have declined from 69 percent in 1998 to 56 percent in 2001. Transportation of cocaine via couriers on commercial flights to and within the United States declined sharply in 2001, according to law enforcement reporting. In addition, reporting indicates that cocaine transportation within the United States via couriers on trains and bus lines decreased in 2001 and that traffickers are increasingly using commercial and private vehicles to transport cocaine in larger shipments. Law enforcement agencies cite increased security at airports, rail stations, and bus terminals as the most likely cause for the shift. Mexican wholesale cocaine distributors have become more active in the New York/New Jersey region. DEA and HIDTA reporting indicates that Mexican criminal groups routinely work with Colombian and Dominican wholesale cocaine distributors directly to supply cocaine from the Southwest Border area to midlevel distributors in the New York/New Jersey region. In fact, the New York/New Jersey HIDTA reports that most cocaine consumed in the New York area is transported via the Southwest Border area by Mexican criminal groups but is distributed by primarily Colombian distribution groups.
ProjectionsCocaine availability and use have been relatively stable, and cocaine will remain a principal drug threat to the country. As cocaine markets expand in Central and South America and in Europe, the average purity of wholesale cocaine transported to U.S. markets will remain lower than the purity levels of the mid-1990s. Continued increases in cocaine production in Colombia, however, and the potential for production levels to increase in Peru and Bolivia may offset the increased demand brought on by market expansion, allowing purity levels to stabilize.
End Notes1. The Office of National Drug Control Policy publishes Pulse Check, a report designed to present findings on drug use patterns and drug markets as reported by ethnographers, epidemiologists, treatment providers, and law enforcement officials. These Pulse Check sources focus on the drug abuse situation in 20 specific sites throughout the country. 2. NDTS data do not imply there is only one drug threat per region. A percentage given for a region represents the proportion of state and local law enforcement agencies in that region that identified a particular drug as their greatest threat. 3. Regions reported in this assessment correspond to the nine Organized Crime and Drug Enforcement Task Force regions. See Figure 1 in Scope and Methodology section. 4. Gangs are defined by the National Alliance of Gang Investigators Associations as groups or associations of three or more persons with a common identifying sign, symbol, or name, the members of which individually or collectively engage in criminal activity that creates an atmosphere of fear and intimidation. 5. NDTS data do not imply that only one drug is available per region. A percentage given for a region represents the proportion of state and local law enforcement agencies in that region that identified a particular drug as available at high, medium, or low levels. 6. The FDSS contains information on drug seizures made by the DEA, Federal Bureau of Investigation, U.S. Customs Service, U.S. Border Patrol, and U.S. Coast Guard. Seizures by other federal agencies are recorded in the FDSS if custody of the drug evidence is transferred to one of those agencies listed. 7. The NHSDA, a project of the Substance Abuse and Mental Health Services Administration since 1971, is the primary source of information on the use of illicit drugs, alcohol, and tobacco by the civilian, noninstitutionalized population in the United States. 8. MTF is an ongoing study of the behaviors, attitudes, and values of students and young adults. Funded by the National Institute on Drug Abuse, MTF annually surveys eighth, tenth, and twelfth graders in public and private schools in the coterminous United States and a subsample of college students and adults from previous graduating classes who participated in the survey as seniors. 9. The PRIDE Survey is the country's largest independent study of adolescent drug use and other behaviors. It presents substance abuse information on sixth through twelfth graders derived from data collected between August and June of the school year. 10. The PATS tracks trends in drug use and drug-related attitudes that drive drug consumption trends. It is the largest ongoing research study of drug-related behaviors and attitudes of children, teens, and adults. 11. DAWN measures the consequences of drug use through hospital emergency departments. Hospitals eligible for DAWN are nonfederal, short-stay, general hospitals in the coterminous United States that have a 24-hour emergency department. DAWN ED data include information on ED episodes that are induced by or related to the use of an illegal drug or the nonmedical use of a legal drug. 12. TEDS provides data on the demographic and substance abuse characteristics of admissions to publicly funded substance abuse treatment programs that report to individual state administrative data systems. 13. The ADAM program measures the extent of drug use in the high-risk population of people who have been arrested. Data are collected through probability-based sampling, and information is derived from interviews and urinalysis obtained voluntarily and recorded confidentially. 14. CEWG is a drug abuse surveillance network established by the National Institute on Drug Abuse and composed of researchers representing 21 areas throughout the country. The CEWG provides current information regarding the nature and patterns of drug abuse, emerging trends, characteristics of vulnerable populations, and social and health consequences. 15. DAWN mortality data include information on drug-induced and drug-related deaths identified and submitted by death investigation jurisdictions participating in DAWN.
|
End of page.