To Contents
To Previous Page
To Next Page
To Publications Page
To Home Page
To Contents
To Previous Page
To Next Page
To Publications Page
To Home Page


U.S. Department of Justice |
The threat posed by the diversion and abuse of CPDs is increasing, largely aided by rapidly increasing distribution of the most addictive CPDs, prescription opioids (see text box). According to DEA, the amount of prescription opioids distributed to retail registrants increased 52 percent from 2003 through 2007.19
|
Prescription Opioids The most commonly diverted CPDs are opioid pain relievers, according to DEA and NSDUH data. Opioid pain relievers are popular among drug abusers because of the euphoria they induce. Opioid pain relievers include codeine, fentanyl (Duragesic, Actiq), hydromorphone (Dilaudid), meperidine (Demerol, which is prescribed less often because of its side effects), morphine (MS Contin), oxycodone (OxyContin), pentazocine (Talwin), dextropropoxyphene (Darvon), methadone (Dolophine), and hydrocodone combinations (Vicodin, Lortab, and Lorcet). Source: Drug Enforcement Administration; Substance Abuse and Mental Health Services Administration. |
Prescription opioid overdose deaths are increasing, primarily because the decedents took the drugs nonmedically,20 other than as prescribed, or in combination with other drugs and/or alcohol.
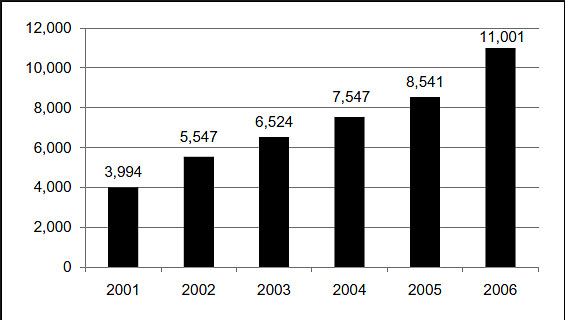
The number of unintentional prescription opioid overdose deaths increased in 2006,21 following a trend that has been apparent since 2000. The overall rate of change from 2002 (5,547 deaths) through 200622 (11,001 deaths) was 98 percent, and the annual rate of change increased during that period (see Figure 18).
Figure 18. Number of Reported Unintentional Poisoning Deaths With Mention of Opioid Analgesics, 2001-2006
Source: Centers for Disease Control and Prevention, National Center
for Health Statistics.
Overdose death data do not provide in-depth information about the decedent's history of drug use or misuse or, in many cases, whether the decedent had a legitimate prescription for the drugs found in his or her system at the time of death. However, CDC reports that a high percentage of people who die from a prescription opioid poisoning have a history of substance abuse and that many have more than one CPD in their system at the time of death. For example, a 2008 CDC study found that 82.3 percent of diversion-related unintentional overdose decedents in West Virginia in 2006 had a history of substance abuse and that 79.3 percent had used multiple substances that contributed to their deaths. In many instances, these individuals were simply using prescription opioids (either singularly or in combination with other CPDs, alcohol, or illicit drugs) to achieve a heroin-like euphoria, and many did not have a legitimate prescription for the drugs. For example, the CDC study found that 63.1 percent of all unintentional CPD overdose deaths in West Virginia in 2006 involved individuals who did not have prescriptions for the drugs that contributed to their deaths.
More law enforcement agencies are reporting that pharmaceutical diversion and abuse pose the greatest drug threat to their areas, in part because of increases in associated crime and gang involvement, which put additional strain on agency budgets and assets.
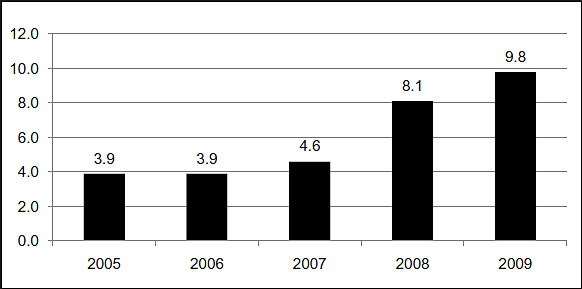
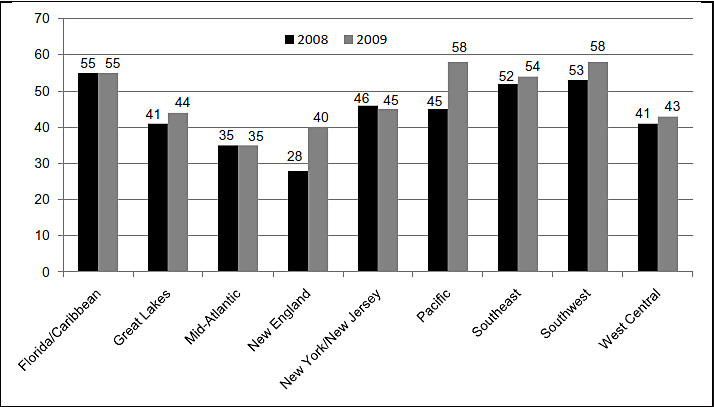
A higher percentage of law enforcement agencies in all nine OCDETF regions responding to the NDTS 2009 reported diverted pharmaceuticals as their greatest drug threat in 2009 than they did in 2008 (see Figure 19). Law enforcement officers base their assessment of the threat on several factors, two of which are diversion- and abuse-related crime rates and gang involvement in drug distribution. For both of these factors, a higher percentage of agencies reported an increase in 2009 (see Table 7). The percentage of agencies reporting that pharmaceutical diversion and abuse contribute to other crime in their areas trended upward in seven of the nine OCDETF regions in 2009 (see Figure 20). The percentage of agencies reporting street gang involvement in pharmaceutical distribution also trended upward in six of the nine OCDETF regions in 2009 (see Figure 21).
Figure 19. Percentage of State and Local Law Enforcement Agencies Reporting CPDs as Their Greatest Drug Threat, 2005-2009
Source: National Drug Threat Survey 2009.
Table 7. Percentage of State and Local Law Enforcement Agencies Reporting Street Gang Involvement in Pharmaceutical Distribution and an Association Between Pharmaceutical Diversion and Crime, 2008-2009
| 2008 | 2009 | |
|---|---|---|
| Street Gang Involvement | 44.2% | 48.0% |
| Property Crime | 6.0% | 8.4% |
| Violent Crime | 3.5% | 4.8% |
Source: National Drug Threat Survey.
Figure 20. Percentage of State and Local Law Enforcement Agencies Reporting an Association Between Pharmaceutical Diversion and Violent and Property Crimes, by OCDETF Region, 2008-2009
Source: National Drug Threat Survey.
Figure 21. Percentage of State and Local Law Enforcement Agencies Reporting Street Gang Involvement in Pharmaceutical Distribution, by OCDETF Region, 2008-2009
Source: National Drug Threat Survey 2009.
Unscrupulous pain clinic physicians in Florida dispense or prescribe large quantities of prescription opioids to dealers and abusers and are a source of supply for opioids distributed in numerous states that have PDMPs.
Nonmedical personnel, primarily investors, are operating numerous purported pain clinics23 in Broward and Palm Beach Counties, Florida. A Florida grand jury found that from 2007 through 2009, the number of pain clinics in those counties grew from 4 to 115, and in one 6-month span, these pain clinic doctors dispensed more than 9 million tablets of oxycodone. The grand jury also found that the Broward and Palm Beach County clinics attract drug seekers from Kentucky, Ohio, Tennessee, and West Virginia.
Unscrupulous physicians--some with criminal records--employed at Florida clinics supply the constant demand for prescription opioids among distributors and abusers in Florida as well as among individuals from states in the Great Lakes, Mid-Atlantic, New England, and Southeast OCDETF Regions, where operational PDMPs have made acquiring CPDs more difficult. These physicians dispense or prescribe large quantities of prescription opioids to customers who have no legitimate need for the drugs; the physicians usually charge an up-front fee for this service and accept only cash payments. Florida law limited what regulators could do with regard to closing clinics or disciplining investors. For example, the Department of Health regulated healthcare professionals but not facilities; the Agency for Health Care Administration provided oversight on clinics that accept insurance, but illegal clinics usually accept only cash. Enacted in July 2009, Florida's new law establishing a PDMP requires that pain management clinics register with the Department of Health. Moreover, under the law, the state medical and osteopathic medicine boards must set standards of practice for all physicians and osteopaths who prescribe controlled substances from those clinics.
|
Recent Cases Involving the Unlawful Dispensing of CPDs A Freeport, Florida, physician was sentenced in January 2009 to 292 months in prison and fined $250,000 after he was found guilty of 43 charges, including healthcare fraud; dispensing controlled substances, including fentanyl, hydrocodone, diazepam, clonazepam, morphine, and alprazolam, the use of which resulted in the death of two persons; and unlawfully dispensing controlled substances, including oxycodone, morphine, fentanyl, hydrocodone, alprazolam, diazepam, clonazepam, and carisoprodol. He also forfeited $260,000 in cash and his medical building for a total civil forfeiture of more than $835,000. The physician had owned and operated a clinic and prescribed CPDs to patients in quantities that made abuse and misuse likely. The physician failed to determine a sufficient medical necessity for the prescribing of these substances. Evidence suggested that he had prescribed controlled substances to patients from across the southeastern United States, knowing that the patients were addicted to the substances, were misusing them, or were doctor-shopping. The manager of two Florida pain management clinics and three prescribing physicians were sentenced in April 2009 for their roles in a prescription drug conspiracy. The manager was sentenced to 240 months in prison; one physician was sentenced to 30 months in prison, and the other two were sentenced to 72 months in prison. The manager of the clinic and the three physicians had purported to provide pain management treatment for chronic pain patients; however, they engaged in a conspiracy to unlawfully dispense hundreds of thousands of controlled pain medications, including OxyContin, Dilaudid, Roxicodone, oxycodone, Lortab, methadone, and others in exchange for cash fees for office visits. The manager was also convicted of possessing, carrying, and using a firearm in the furtherance of the conspiracy. Federal law enforcement authorities in November 2009 dismantled a Florida trafficking ring that had sent more than 190,000 oxycodone tablets from South Florida pain clinics to abusers in Kentucky, North Carolina, Tennessee, Virginia, and West Virginia. At least 20 people were indicted on distribution charges; the ring had allegedly operated for 3 years and used at least four or five clinic doctors per day to obtain the drugs. Members of the ring shipped thousands of pills per day by vehicle or overnight delivery services and allegedly made at least $5 million over the 3 years. Kentucky State Police detectives and troopers along with FBI agents, armed with 518 felony arrest warrants, conducted a drug roundup in October 2009 that stemmed from Operation Flamingo Road. This investigation targeted Kentucky drug traffickers in at least 33 counties who had traveled to South Florida to obtain CPDs from pain clinic doctors and returned to Kentucky to distribute the drugs. Penalties for felony charges of trafficking in controlled substances range from 18 months to 20 years in prison. |
19.
The narcotic raw material produced in or imported
into the United States is subject to an annual assessment of legitimate medical,
scientific, and research need and the establishment of quotas by DEA. Contributing
factors to quota increases include: more aggressive pain treatment, new and different
indications for legitimate medical use, the increase in the average age of the citizenry,
new delivery methods and formulations for opioid pain relievers, new product development,
and exportation. Thus, decreased production is not viewed as a realistic means to
reduce diversion.
20.
Nonmedical use involves obtaining the drugs without
a legitimate prescription and taking them while not under medical supervision.
21.
Prescription opioid death data for 2006 are the
most current estimates.
22.
The 2006 data include more than 1,000 overdose
deaths attributed to heroin and clandestinely produced fentanyl that was distributed
in some Midwest, Great Lakes, and Mid-Atlantic cities.
23.
DEA investigations indicate that dubious pain clinics
have unique characteristics, some of which include the ability to quickly relocate,
vague or misleading ownership records, form nearly exclusive association with specific
pharmacies, use specific physicians, cash-based payment methods, and rapid examinations.
UNCLASSIFIED
End of page.